Acute coronary syndrome or ACS is defined as a sudden, reduced blood flow to the heart. ACS is seen in ST-segment elevation myocardial infarction (STEMI), non-ST- egment elevation myocardial infarction (NSTEMI) or unstable angina. Myocardial ischemia occurs when there is not enough blood supply to the heart muscle and that results from coronary artery disease (CAD). ACS is usually caused by atherosclerosis and coronary thrombosis, but can also be associated with cocaine use. Other conditions that cause ACS include:
Unstable Angina (UA)
Microemboli
Occlusive Thrombus
Unstable Plaque
The symptoms associated with ACS include:
Chest pain radiating to the left arm and left angle of jaw
Shortness of breath
Nausea
Vomiting
Diaphoresis
Palpitations
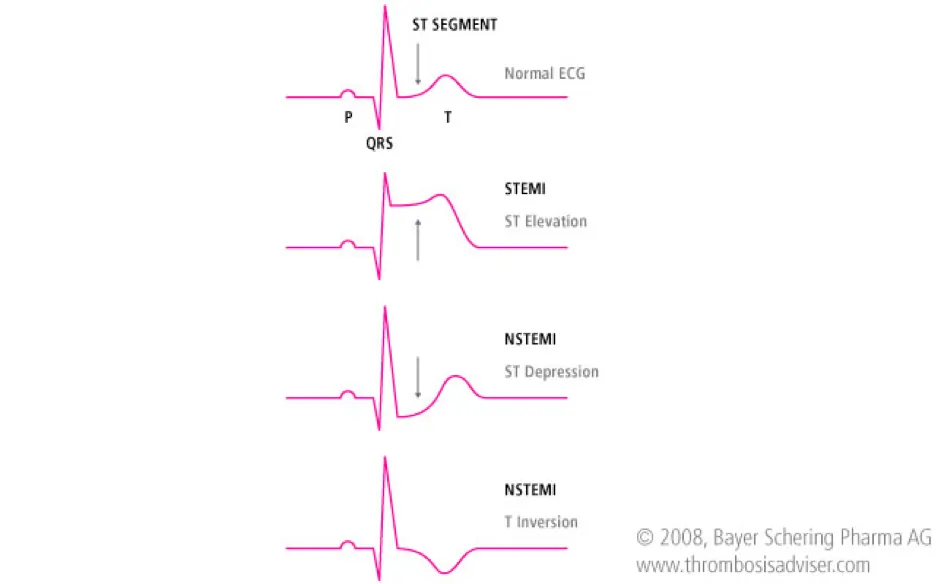
ST-Segment Elevation Myocardial Infarction (STEMI) is an elevation > 1mm in 2 or more contiguous or greater than 2 mm in leads V2 and V3. Unstable Angina (UA) or Non ST-Elevation Myocardial Infarction (NSTEMI) is a depression ≥0.5 mm or greater T-wave inversion. Low Risk Unstable Angina (UA) is an ST segment deviation of <0.5 mm or T wave inversion of 2 mm. Patients may also have normal ECGs.
Asystole can be caused by many factors and are represented as H’s and T’s:
Scenario: A 70-year patient comes to the hospital and is complaining of chest pain radiating to his arm and he seems very anxious and out of breath. Assessment:
Identify signs and symptoms of ischemia or infarction
Monitor vital signs and cardiac rhythm
Be prepared to do CPR and use the AED
IV access
Check cardiac markers, electrolytes and coagulation status
Interventions:
Give aspirin (162 – 325 mg), oxygen if O2 saturation is <90%, start oxygen at 4L/min, start oxygen at 4L/min, nitroglycerin sublingual every 3 to 5 minutes, and morphine for pain.
Be mindful of inferior wall myocardial infarction (MI) and right ventricular (RV) infarction.
Monitor for systolic blood pressure (SBP) below 90mmHg and significant bradycardia (heart rate less then 50/min), or marked tachycardis.
Caution with phosphodiesterase inhibitor usage due to the potential for severe hypotension.
Conduct a 12-lead ECG and diagnose
Management:
If STEMI on ECG perform rapid fibrinolytic therapy (“clot buster”) or direct reperfusion
If time of onset of symptoms is ≤12 hours – reperfusion:
Door to balloon inflation (PCI) – 90 minutes
Door to needle fibrinolysis – 30 minutes
If time of onset of symptoms is >12 hours, then invasive treatment is recommended
If high risk UA or NSTEMI on ECG check troponin level and start invasive treatment
Immediate medications are
Aspirin
Nitroglycerin
Morphine
Consideration of p2y12 inhibitors (antiplatelet)
Monitor and continue heparin and may add ACE inhibitor and HMG CoA reductase inhibitors if needed
If low risk ACS check cardiac markers, repeat ECG, conduct non-invasive diagnostic test
If no ischemia or infarction discharge and schedule a follow-up
Treatments which are used in ACLS algorithm for ACS are:
Oxygen
Aspirin
Nitroglycerin
Morphine
Fibrinolytic (thrombolytic) therapy
Heparin
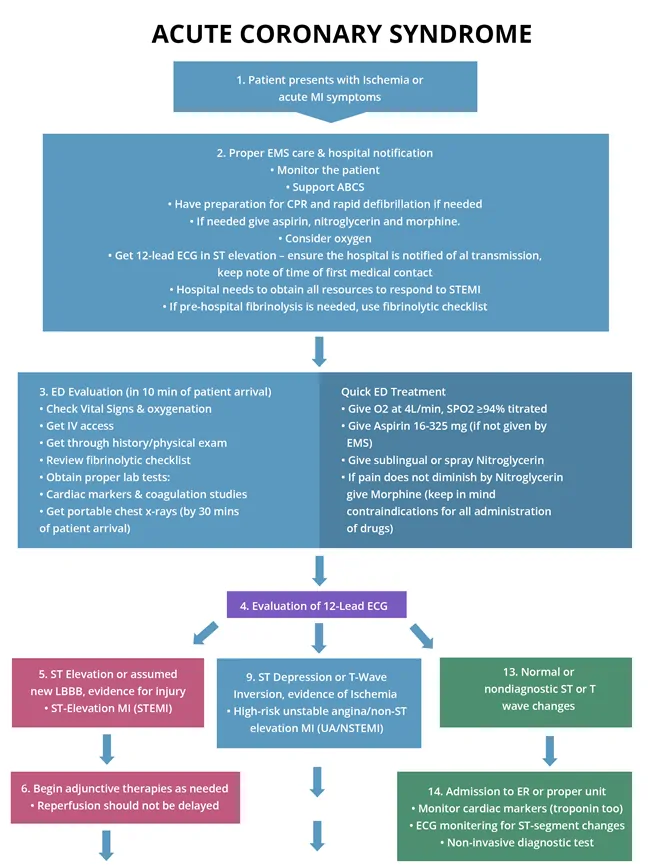
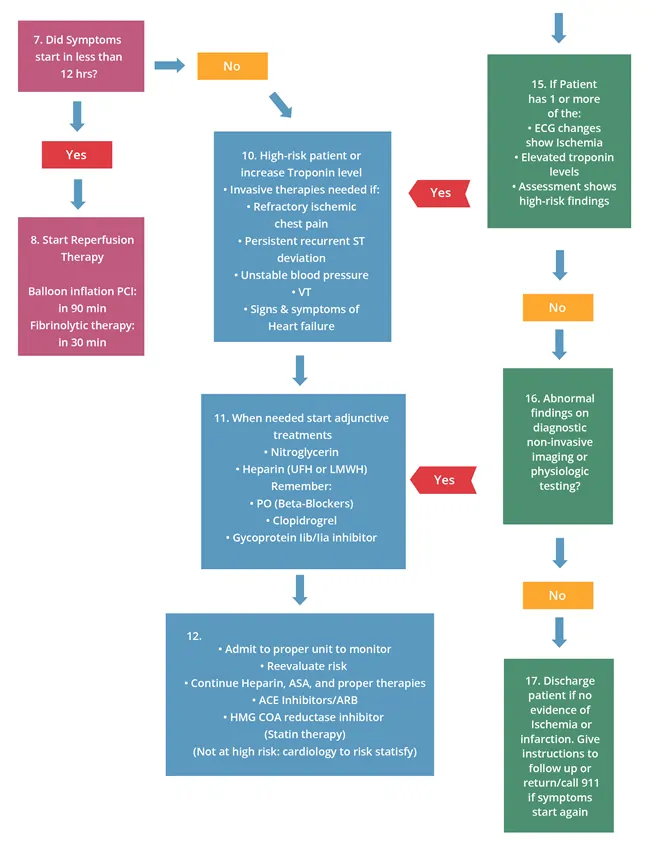
The following is an algorithm that shows management of ACS in detail: