Tachycardia is when the heart rate or rhythm is too fast (>100 beats/min). Increase in heart rate causes less blood to be pumped through the systemic and pulmonary systems. Low blood flow will cause less oxygen to flow to the heart and brain and less oxygen to the heart can lead to Ischemia and MI. Unstable tachycardia is when the heart rate is too fast causing unstable conditions and symptoms caused by >150bpm. Some symptoms may include:
Hypotension
Altered mental status
Shock
Chest pain or discomfort
Acute heart failure
The rhythms for unstable tachycardia include:
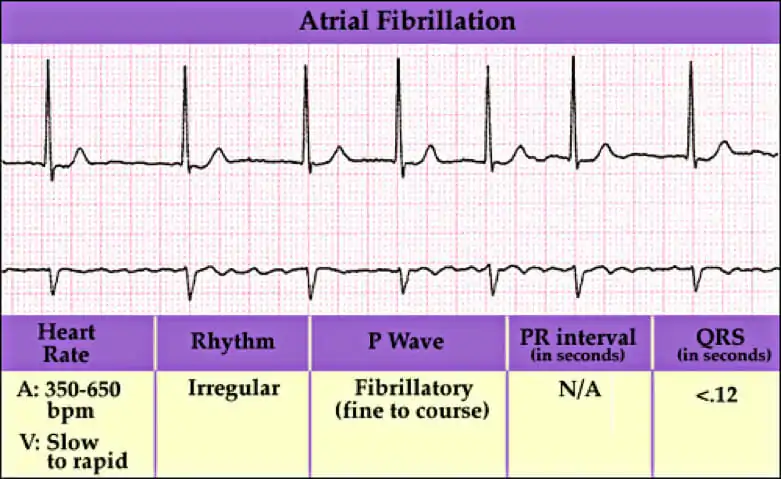
Atrial fibrillation
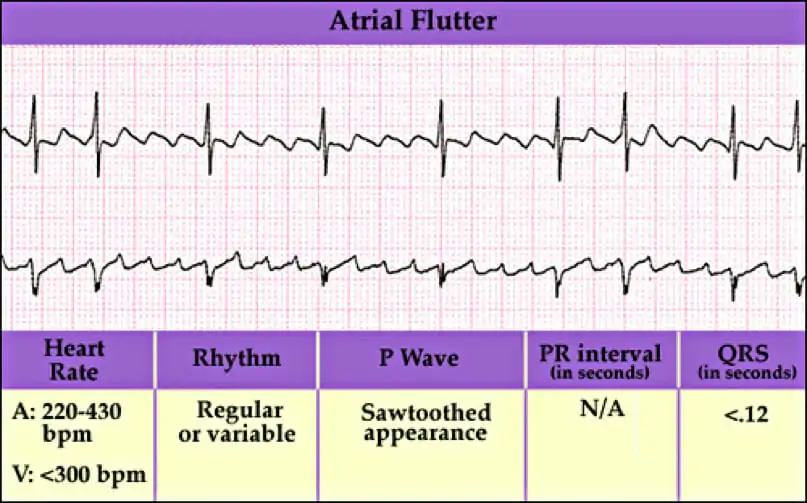
Atrial flutter
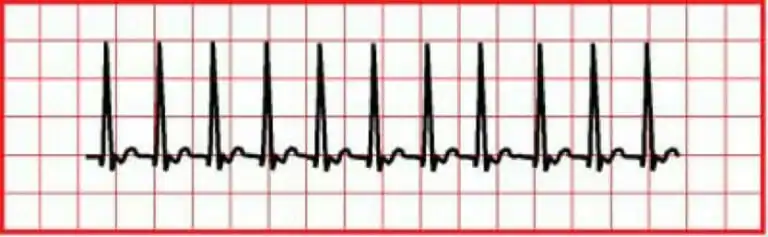
SVT
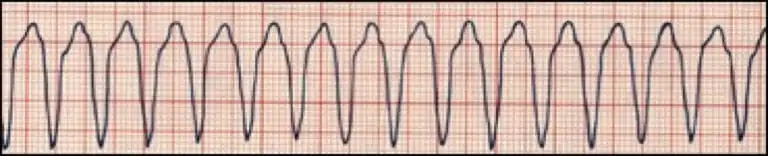
Monomorphic VT
Polymorphic VT
Wide-Complex tachycardia of uncertain type
Atrial fibrillation is when the heart beats do not occur at the same intervals. It is known as the quivering of the muscles and involves both the atriums of the heart.
Atrial flutter is abnormal heart rhythm causing fast irregular heartbeat. Starts in the atrium and can lead to atrial fibrillation. Usually has a ‘saw-toothed’ appearance.
Supraventricular Tachycardia (SVT) is a rapid and narrow heartbeat that starts in the atria or AV node.
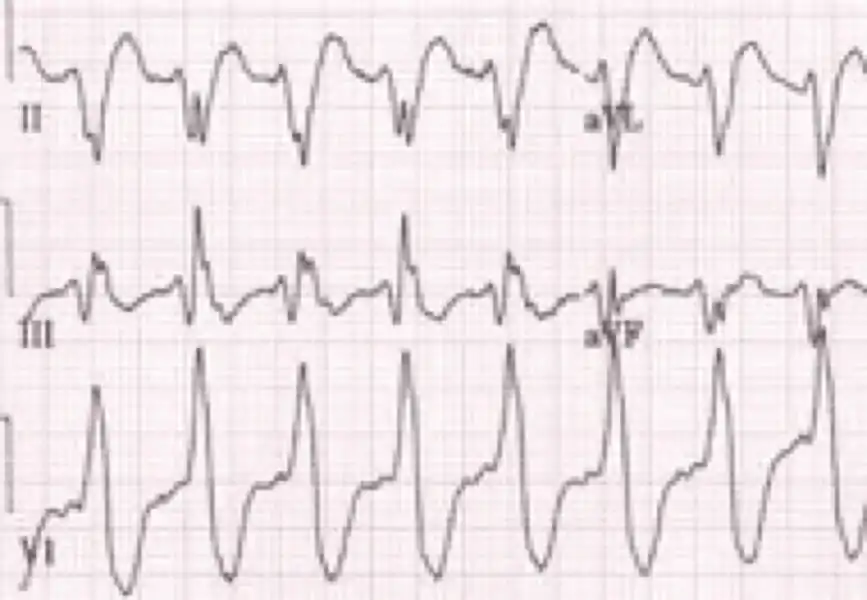
Monomorphic VT is heart rate of >150 bpm but all QRS look the same.
Polymorphic VT is when different areas in the ventricles fire fast, uncoordinated impulses.
Wide-complex tachycardia is due to ventricular tachycardia or SVT with wide QRS complex (at least 0.12 seconds).
Scenario: A 45 year old patient arrives to the hospital with chest pain and palpatations. As the nurse was obtaining medical history and checking vital signs the patient faints for a few minutes.
Assessment:
Check for responsiveness – Tap and shout “Are you alright?” and look at chest for movement. Check carotid pulse and note there is pulse and breathing
Put the patient on a monitor and identify Tachycardia (>100 beats/min)
Call the doctor on duty
Interventions:
Maintain airway
Help with breathing and give oxygen if hypoxemic and monitor O2 saturation
Monitor BP and HR and conduct a 12-lead ECG and diagnose
Check for persistent tachyarrhythmia
Management: at the hospital
If persistent tachyarrhythmia initiate synchronized cardioversion
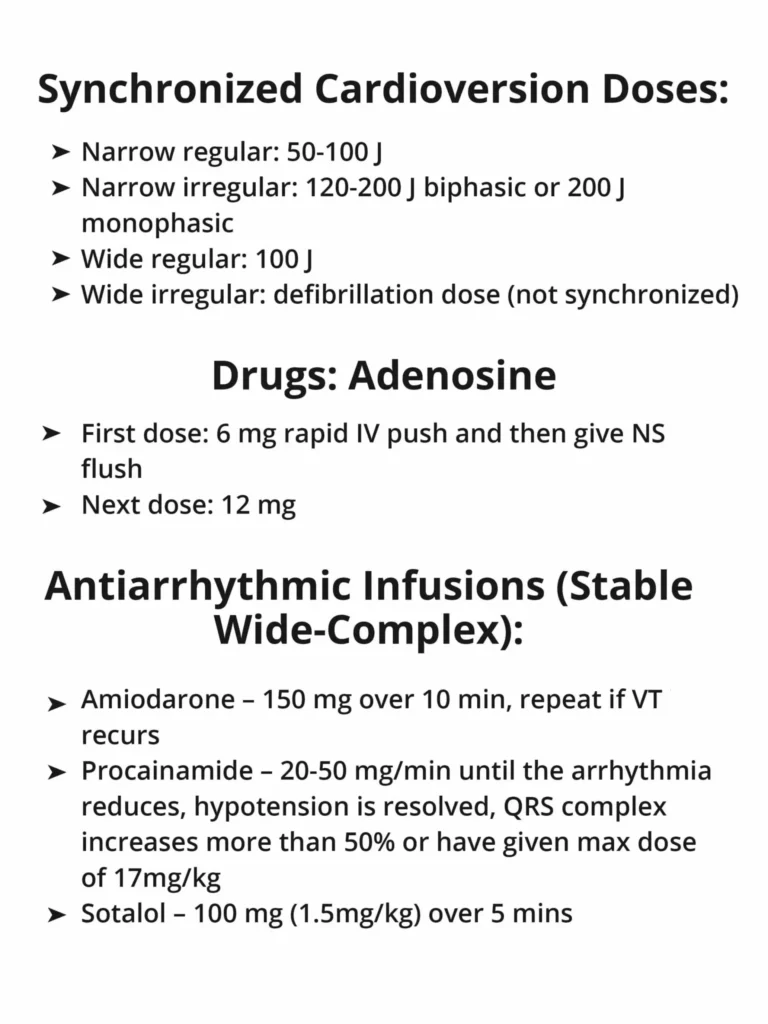
Narrow regular 50-100 J
Narrow irregular 120-200 J biphasic and 200 J monophasic
Wide regular 100 J
Wide irregular defibrillation dose
Administer Adenosine IV dose 6mg rapid IV push with NS flush and 12 mg for second dose
If not persistent tachyarrythmia and if wide QRS ≥12 seconds then obtain IV access and 12-lead ECG
Administer Adenosine if monomorphic
Administer antiarrhythmic infusion (Procaainaminde, Amiodorone, Sotalol)
If not irregular wide QRS consider: vagal maneuvers, adenosine, beta blockers, calcium channel blockers
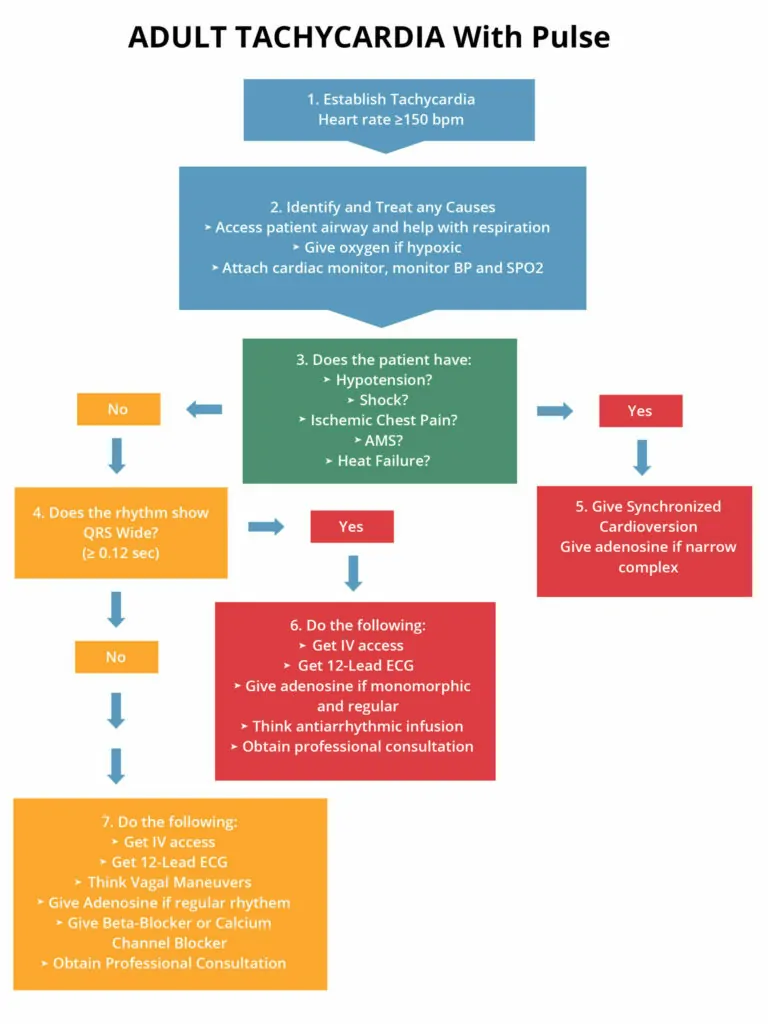
The following is an algorithm showing management of unstable tachycardia in detail:
Cardioversion
Synchronized cardioversion is used during unstable tachycardia, but there may be times when unsynchronized cardioversion will need to be used.
Synchronized cardioversion needs to be used with:
Unstable SVT
Unstable atrial fibrillation
Unstable atrial flutter
Unstable regular monomorphic tachycardia with a pulse
Unsynchronized cardioversion needs to be used with:
No pulse
Critical issues – patient going into cardiac arrest
Patient in monomorphic or polymorphic VT
Patient at risk of going into arrest
Energy in Joules used during cardioversion:
Rhythm
First Dose (Monophasic Defibrillator)
Unstable atrial fibrillation
200 J
Unstable Monomorphic VT
100 J
Other unstable SVT, Atrial Flutter
200 J
Unstable polymorphic VT (irregular form & rate)
Use like VF with high-energy shock (360J)
How to Give Synchronized Cardioversion
Anesthetize patient unless they are crashing or unstable
Turn on the defibrillator
Put the leads on the patient and ensure the rhythm is on the monitor. Put on the adhesive electrode pads on the patient
Push the SYNC button to get to the synchronized mode
Ensure the markers are on the R wave – this shows that the sync mode is on
Pick the correct energy level
Ensure everyone is clear – “Stand clear, charging defibrillator!”
Push the charge button
Again clear patient – “Everyone Clear!”
Push the shock button
Check rhythm to see if tachycardia is still present. If tachycardia is persistent, increase energy level slowly
Press SYNC button again to activate the sync mode
Learning Outcomes:
You have completed Chapter XI. Now you should be able to:
Recognize the types of ECG rhythms associated with Tachycardia
Apply the Adult Tachycardia Algorithm in Unstable Tachycardia
Understand the signs & symptoms of Tachycardia
Understand synchronized and unsynchronized cardioversion